(七)治疗过程中监测 启动治疗12周时,应监测血清HBV DNA水平,以评价其治疗应答;24周时监测血清HBV DNA水平,以确证是否获得病毒学应答。治疗第1年,应每3~6个月监测HBV DNA水平,以确认是良好的病毒学抑制或病毒学突破。 1. 原发性治疗失败 对于原发性治疗失败,AASLD 2018年慢性乙肝指南的定义是:治疗6个月HBV DNA下降[16];EASL 2017年慢性乙肝指南的定义是:治疗3个月HBV DNA下降[17]。 该《流程》指出:ETV、TDF和TAF治疗慢性乙肝患者发生原发性无应答少见,对治疗12~24周无应答患者,应评价其依从性;对依从性好的患者,治疗24周时应检测耐药,以确定针对耐药变异株的最佳救治策略。 2. 部分病毒学应答或应答不佳 部分病毒学应答的定义指治疗至24周HBV DNA≥2000 IU/ml或治疗至48周HBV DNA仍可检测到。该《流程》指出,对部分应答或应答欠佳的患者,应评价其依从性。用ETV、TDF或TAF治疗慢性乙肝48周时还可检测到HBV DNA的患者的最佳管理策略尚不清楚。对于血清HBV DNA呈下降的患者,可继续用ETV或TDF治疗,病毒学应答率可随治疗时间延长而升高,发生耐药的风险很低[53-54]。用ETV治疗1年后HBV DNA[55]。另一治疗策略是:对ETV治疗1年部分应答的患者,换用TDF或TAF单药治疗,或与TDF或TAF加ETV联合治疗[56]。有研究报道,用0.5 mg/d ETV治疗部分应答的慢性乙肝患者,增加ETV剂量至1 mg/d不能达到完全病毒学抑制[57]。 3. 病毒学耐药监测 病毒学耐药在临床上为病毒学突破,其定义是:患者有病毒学应答且依从性好,但血清HBV DNA检测2次,间隔1个月, 较原应答的HBV DNA下限上升1 log IU/ml[58]。该《流程》指出,ETV治疗5年耐药发生率为1.2%,TDF和TAF未报告耐药。临床上大量耐药是依从性差所致,真正耐药发生率低[59-60](表 2)。 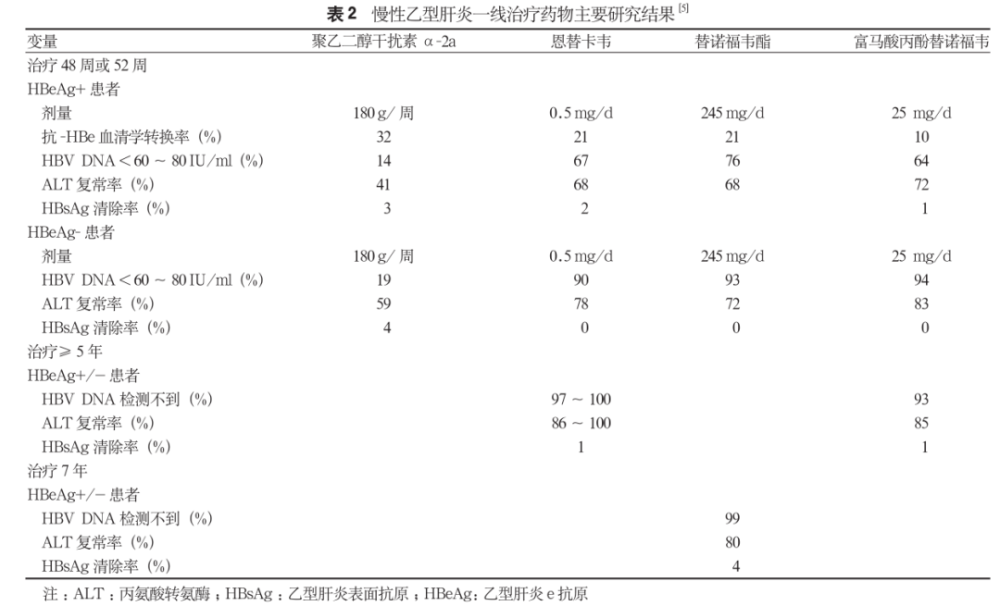
耐药管理的推荐意见不一[61-63],但一般是加用或换用不同种类的药。在临床上,对怀疑ETV耐药的患者,推荐用TDF或TAF单药治疗。对合并人类免疫缺陷病毒感染患者,选择TAF 25 mg/d和恩曲他滨200 mg/d治疗。 四、结论 制订该《流程》的专家组预计,虽然有多种药物正在临床研发中,但在未来几年内,现已获批的药物仍将是治疗慢性乙肝的唯一选择。同时专家组认为,接下来的重要目标是努力识别HBV感染患者和继续重新评估每例患者是否需要抗病毒治疗。 参考文献:(向下滑动,查看全部文献) [1] Keeffe EB, Dieterich DT, Han S-HB, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States[J]. Clin Gastroenterol Hepatol, 2004, 2(2): 87-106. DOI:10.1016/s1542-3565(03)00312-4. [2] Keeffe EB, Dieterich DT, Han S-HB, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: an update[J]. Clin Gastroenterol Hepatol, 2006, 4(8): 936-962. DOI: 10.1016/j.cgh.2006.05.016. [3] Keeffe EB, Dieterich DT, Han S-HB, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update[J]. Clin Gastroenterol Hepatol, 2008, 6(12):1315-1341. DOI: 10.1016/j.cgh.2008.08.021. [4] Martin P, Lau DTY, Nguyen MH, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2015 update[J]. Clin Gastroenterol Hepatol, 2015, 13(12): 2071-2087.e16. DOI: 10.1016/j.cgh.2015.07.007. [5] Martin P, Nguyen MH, Dieterich DT, et al. Treatment algorithm for managing chronic hepatitis B virus infection in the United States:2021 update[J]. Clin Gastroenterol Hepatol, 2021, 27: S1542-3565(21)00818-1. DOI: 10.1016/j.cgh.2021.07.036. [6] Roberts H, Kruszon-Moran D, Ly KN, et al. Prevalence of chronic hepatitis B virus (HBV) infection in U.S. households: National Health and Nutrition Examination Survey (NHANES), 1988-2012[J]. Hepatology, 2016, 63(2): 388-397. DOI: 10.1002/hep.28109. [7] Nguyen VH, Le AK, Trinhet HN, et al. Poor adherence to guidelines for treatment of chronic hepatitis B virus infection at primary care and referral practices[J]. Clin Gastroenterol Hepatol, 2019,17(5): 957-967.e7. DOI: 10.1016/j.cgh.2018.10.012. [8] Chen VL, Yeh ML, Le AK, et al. Anti-viral therapy is associated with improved survival but is underutilised in patients with hepatitis B virus-related hepatocellular carcinoma: real-world east and west experience[J] Aliment Pharmacol Ther, 2018, 48(1): 44-54. DOI: 10.1111/apt.14801. [9] Ogawa E, Yeo YH, Dang N, et al. Diagnosis rates of chronic hepatitis B in privately insured patients in the United States[J]. JAMA Netw Open, 2020, 3(4): e201844. DOI: 10.1001/ jamanetworkopen.2020.1844. [10] Buti M, Gane E, Seto WK, et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of patients with HBeAg-negative chronic hepatitis B virus infection: a randomised, double-blind, phase 3, non-inferiority trial[J]. Lancet Gastroenterol Hepatol, 2016, 1(3): 196-206. DOI: 10.1016/S2468-1253(16)30107-8. [11] Chan HLY, Fung S, Seto WK, et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of HBeAg-positive chronic hepatitis B virus infection: a randomised, double-blind, phase 3, non-inferiority trial[J]. Lancet Gastroenterol Hepatol, 2016,1(3): 185-195. DOI: 10.1016/S2468-1253(16)30024-3. [12] Toyoda H, Leong J, Landis C, et al. Treatment and renal outcomes up to 96 weeks after tenofovir alafenamide switch from tenofovir disoproxil fumarate in routine practice[J]. Hepatology, 2021, 74(2):656-666. DOI: 10.1002/hep.31793. [13] Mason WS, Gill US, Litwin S, et al. HBV DNA integration and clonal hepatocyte expansion in chronic hepatitis B patients considered immune tolerant[J]. Gastroenterology, 2016, 151: 986-998.e4. DOI: 10.1053/j.gastro.2016.07.012. [14] Liu A, Le A, Zhang J, et al. Increasing co-morbidities in chronic hepatitis B patients: experience in primary care and referral practices during 2000-2015[J]. Clin Tranl Gastroenterol, 2018, 9(3): 141.DOI: 10.1038/s41424-018-0007-6. [15] Tan M, Bhadoria AS, Cui F, et al. Estimating the proportion of people with chronic hepatitis B virus infection eligible for hepatitis B antiviral treatment worldwide: a systematic review and meta-analysis[J]. Lancet Gastroenterol Hepatol, 2021, 6: 106-119. DOI: 10.1016/S2468-1253(20)30307-1. [16] Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance[J]. Hepatology, 2018, 67(4): 1560-1599. DOI:10.1002/hep.29800. [17] European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection[J]. J Hepatol, 2017, 67(2): 370-398. DOI: 10.1016/j.jhep.2017.03.021. [18] Kennedy PTF, Litwin S, Dolman GE, et al. Immune tolerant chronic hepatitis B: the unrecognized risks[J]. Viruses, 2017, 9(5): 96. DOI: 10.3390/v9050096. [19] Chan HL-Y, Wong ML, Hui AY, et al. Hepatitis B virus genotype C takes a more aggressive disease course than hepatitis B virus genotype B in hepatitis B e antigen-positive patients[J]. J Clin Microbiol, 2003, 41(3): 1277-1279. DOI: 10.1128/JCM.41.3.1277-1279.2003 [20] Chu C-M, Liaw Y-F. Predictive factors for reactivation of hepatitis B following hepatitis B e antigen seroconversion in chronic hepatitis B[J]. Gastroenterology, 2007, 133(5): 1458-1465. DOI: 10.1053/j.gastro.2007.08.039. [21] Wong GLH, Chan HLY, Yiu KKL, et al. Meta-analysis: the association of hepatitis B virus genotypes and hepatocellular carcinoma[J]. Aliment Pharmacol Ther, 2013, 37(5): 517-526. DOI:10.1111/apt.12207. [22] Yang HI, Yeh SH, Chen PJ, et al. Associations between hepatitis B virus genotype and mutants and the risk of hepatocellular carcinoma[J]. J Natl Cancer Inst, 2008, 100(16): 1134-1143. DOI:10.1093/jnci/djn243. [23] Babusis D, Phan TK, Lee WA, et al. Mechanism for effective lymphoid cell and tissue loading following oral administration of nucleotide prodrug GS-7340[J]. Mol Pharm, 2013, 10(2): 459-466.DOI: 10.1021/mp3002045. [24] Murakami E, Wang T, Park Y, et al. Implications of effi cient hepatic delivery by tenofovir alafenamide (GS-7340) for hepatitis B virus therapy[J]. Antimicrob Agents Chemother, 2015, 59(6): 3563-3569.DOI: 10.1128/AAC.00128-15. [25] Agarwal K, Fung SK, Nguyen TT, et al. Twenty-eight day safety, antiviral activity, and pharmacokinetics of tenofovir alafenamide for treatment of chronic hepatitis B infection[J]. J Hepatol, 2015, 62(3):533-540. DOI: 10.1016/j.jhep.2014.10.035. [26] Ruane PJ, DeJesus E, Berger D, et al. Antiviral activity, safety, and pharmacokinetics/ pharmacodynamics of tenofovir alafenamide as 10-day monotherapy in HIV-1-positive adults[J]. J Acquir Immune Def Syndr, 2013, 63: 449-455. DOI: 10.1097/ QAI.0b013e3182965d45. [27] Lampertico P, Buti M, Fung S, et al. Switching from tenofovir disoproxil fumarate to tenofovir alafenamide in virologically suppressed patients with chronic hepatitis B: a randomised,double-blind, phase 3, multicentre non-inferiority study[J]. Lancet Gastroenterol Hepatol, 2020, 5(5): 441-353. DOI: 10.1016/S2468-1253(19)30421-2. [28] Toyoda H, Leong J, Landis C, et al. Treatment and renal outcomes up to 96 weeks after tenofovir alafenamide switch from tenofovir disoproxil fumarate in routine practice[J]. Hepatology, 2021, 74(2):656-666. DOI: 10.1002/hep.31793. [29] Nguyen MH, Atsukawa M, Ishikawa T, et al. Outcomes of sequential therapy with tenofovir alafenamide after long-term entecavir[J]. Am J Gastroenterol, 2021, 116(6): 1264-1273. DOI: 10.14309/ajg.0000000000001157. [30] Marcellin P, Ahn SH, Ma X, et al. Study 149 investigators. combination of tenofovir disoproxil fumarate and peginterferon a-2a increases loss of hepatitis B surface antigen in patients with chronic hepatitis B[J]. Gastroenterology, 2016, 150(1): 134-144. DOI: 10.1053/j.gastro.2015.09.043. [31] Liaw YF, Jia JD, Chan HLY, et al. Shorter durations and lower doses of peginterferon alfa-2a are associated with inferior hepatitis B e antigen seroconversion rates in hepatitis B virus genotypes B or C[J]. Hepatology, 2011, 54(5): 1591-1599. DOI: 10.1002/hep.24555. [32] Cao ZH, Ma LN, Zhang HW, et al. Extended treatment with peginterferon a-2a in combination with lamivudine or adefovir for 96 weeks yields high rates of HBeAg and HBsAg seroconversion[J]. J Dig Dis, 2013, 14(8): 446-450. DOI: 10.1111/1751-2980.12065 [33] Lampertico P, Viganò M, Di Costanzo GG, et al. Randomised study comparing 48 and 96 weeks peginterferon a-2a therapy in genotype D HBeAg-negative chronic hepatitis B[J]. Gut, 2013, 62(2): 290-298. DOI: 10.1136/gutjnl-2011-301430. [34] Sonneveld MJ, Hansen BE, Piratvisuth T, et al. Responseguided peginterferon therapy in hepatitis B e antigen-positive chronic hepatitis B using serum hepatitis B surface antigen levels[J].Hepatology, 2013, 58(3): 872-880. DOI: 10.1002/hep.26436. [35] Sonneveld MJ, Rijckborst V, Boucher CAB, et al. Prediction of sustained response to peginterferon alfa-2b for hepatitis B e antigen-positive chronic hepatitis B using on-treatment hepatitis B surface antigen decline[J]. Hepatology, 2010, 52(4): 1251-1257. DOI: 10.1002/hep.23844. [36] Rijckborst V, Hansen BE, Cakaloglu Y, et al. Early on-treatment prediction of response to peginterferon alfa-2a for HBeAg negative chronic hepatitis B using HBsAg and HBV DNA levels[J]. Hepatology, 2010, 52(2): 454-461. DOI: 10.1002/hep.23722. [37] Rijckborst V, Hansen BE, Ferenci P, et al. Validation of a stopping rule at week 12 using HBsAg and HBV DNA for HBeAg negative patients treated with peginterferon alfa-2a[J]. J Hepatol, 2012, 56(5):1006-1011. DOI: 10.1016/j.jhep.2011.12.007 [38] Reijnders JGP, Perquin MJ, Zhang N, et al. Nucleos(t)ide analogues only induce temporary hepatitis B e antigen seroconversion in most patients with chronic hepatitis B[J]. Gastroenterology, 2010, 139(2):491-498. DOI: 10.1053/j.gastro.2010.03.059. [39] Chaung KT, Ha NB, Trinh HN, et al. High frequency of recurrent viremia after hepatitis B e antigen seroconversion and consolidation therapy[J]. J Clinical Gastroenterol, 2012, 46(10): 865-870. DOI:10.1097/MCG.0b013e31825ceed9. [40] Papatheodoridis G, Rigopoulou E, Papatheodoridi M, et al. DARING-B: discontinuation of effective entecavir or tenofovir therapy in non-cirrhotic HBeAg-negative chronic hepatitis B patients: a prospective Greek study[J]. J Hepatol, 2017, 66(Suppl 1):S26. [41] Ha NB, Ha NB, Garcia RT, et al. Renal dysfunction in chronic hepatitis B patients treated with adefovir dipivoxil[J]. Hepatology, 2009, 50(3): 727-734. DOI: 10.1002/hep.23044. [42] Gilead Sciences. Prescribing information for vemlidy[EB/OL]. Available at: https://www.gilead.com/-/media/f ... idy/vemlidy_pi.pdf. Accessed February 15, 2021. [43] Weinstein JR, Anderson S. The aging kidney: physiological changes[J]. Adv Chronic Kidney Dis, 2010, 17(4): 302-307. DOI:10.1053/j.ackd.2010.05.002. [44] Nguyen MH, Lim JK, Burak Ozbay A, et al. Advancing age and comorbidity in a US insured population-based cohort of patients with chronic hepatitis B[J]. Hepatology, 2019, 69(3): 959-973. DOI:10.1002/hep.30246 [45] Wong GL, Wong VW, Yuen BW, et al. An aging population of chronic hepatitis B with increasing comorbidities: a territory-wide study from 2000 to 2017[J]. Hepatology, 2020, 71(2): 444-455. DOI:10.1002/hep.30833. [46] Oh H, Jun DW, Lee IH, et al. Increasing comorbidities in a South Korea insured population-based cohort of patients with chronic hepatitis B[J]. Aliment Pharmacol Ther, 2020, 52(2): 371-381. DOI:10.1111/apt.15867. [47] Tseng CH, Hsu YC, Ho HJ, et al. Increasing age and nonliver comorbidities in patients with chronic hepatitis B in Taiwan: a nationwide population-based analysis[J]. Dig Dis, 2021, 39(3): 266-274. DOI: 10.1159/000511585. [48] Yotsuyanagi H, Kurosaki M, Yatsuhashi H, et al. Characteristics and healthcare costs in the aging hepatitis B population of Japan: a nationwide real-world analysis[J]. Dig Dis, 2022, 40(1): 68-77. DOI:10.1159/000515854. [49] Gara N, Zhao X, Collins MT, et al. Renal tubular dysfunction during long-term adefovir or tenofovir therapy in chronic hepatitis B[J]. Aliment Pharmacol Ther, 2012, 35(11): 1317-1325. DOI: 10.1111/j.1365-2036.2012.05093.x. [50] Chen YC, Su YC, Li CY, et al. A nationwide cohort study suggests chronic hepatitis B virus infection increases the risk of end-stage renal disease among patients in Taiwan[J]. Kidney Int, 2015, 87(5):1030-1038. DOI: 10.1038/ki.2014.363. [51] Center JR, Nguyen TV, Schneider D, et al. Mortality after all major types of osteoporotic fracture in men and women: an observational study[J]. Lancet, 1999, 353(9156): 878-882. DOI: 10.1016/S0140-6736(98)09075-8. [52] Prasad D, Nguyen MH. Chronic hepatitis, osteoporosis, and men: under-recognised and underdiagnosed[J]. Lancet Diabetes Endocrinol, 2021, 9(3): 141. DOI: 10.1016/S2213-8587(21)00020-6. [53] Gordon SC, Krastev Z, Horban A, et al. Efficacy of tenofovir disoproxil fumarate at 240 weeks in patients with chronic hepatitis B with high baseline viral load[J]. Hepatology, 2013, 58(2): 505-513.DOI: 10.1002/hep.26277. [54] Yang YJ, Shim JH, Kim KM, et al. Assessment of current criteria for primary nonresponse in chronic hepatitis B patients receiving entecavir therapy[J]. Hepatology, 2014, 59(4): 1303-1310. DOI:10.1002/hep.26910. [55] Zoutendijk R, Reijnders JGP, Brown A, et al. Entecavir treatment for chronic hepatitis B: adaptation is not needed for the majority of na ve patients with a partial virological response[J]. Hepatology,2011, 54(2): 443-451. DOI: 10.1002/hep.24406. [56] Lu L, Yip B, Trinh H, et al. Tenofovir-based alternate therapies for chronic hepatitis B patients with partial virological response to entecavir[J]. J Viral Hepat, 2015, 22(8): 675-681. DOI: 10.1111/jvh.12368 [57] Ha NB, Ha NB, Trinh HN, et al. Response to higher dose of entecavir 1.0 mg daily in patients with partial response to entecavir 0.5 mg daily[J]. J Clin Gastroenterol, 2013, 47(5): 461-465. DOI:10.1097/MCG.0b013e318266fd31. [58] Lok AS, Zoulim F, Locarnini S, et al. Antiviral drug-resistant HBV: standardization of nomenclature and assays and recommendations for management[J]. Hepatology, 2007, 46(1): 254-265. DOI:10.1002/hep.21698. [59] Ha NB, Ha NB, Garcia RT, et al. Medication nonadherence with long-term management of patients with hepatitis B e antigen negative chronic hepatitis B[J]. Dig Dis Sci, 2011, 56(8): 2423-2431.DOI: 10.1007/s10620-011-1610-5. [60] Hongthanakorn C, Chotiyaputta W, Oberhelman K, et al. Virological breakthrough and resistance in patients with chronic hepatitis B receiving nucleos(t)ide analogues in clinical practice[J]. Hepatology,2011, 53(6): 1854-1863. DOI: 10.1002/hep.24318. [61] Lok ASF, McMahon BJ. Chronic hepatitis B: update 2009[J]. Hepatology, 2009, 50(3): 661-662. DOI: 10.1002/hep.23190 [62] European Association for The Study of The Liver. EASL clinical practice guidelines: management of chronic hepatitis B virus infection[J]. J Hepatol, 2012, 57(1): 167-185. DOI: 10.1016/j.jhep.2012.02.010 [63] Liaw Y-F, Kao J-H, Piratvisuth T, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2012 update[J]. Hepatol Int, 2012, 6(3): 531-561. DOI: 10.1007/s12072-012-9365-4. | 




 发表于 2022-8-2 11:42
发表于 2022-8-2 11:42