|

- 现金
- 62111 元
- 精华
- 26
- 帖子
- 30441
- 注册时间
- 2009-10-5
- 最后登录
- 2022-12-28

|
Discussion
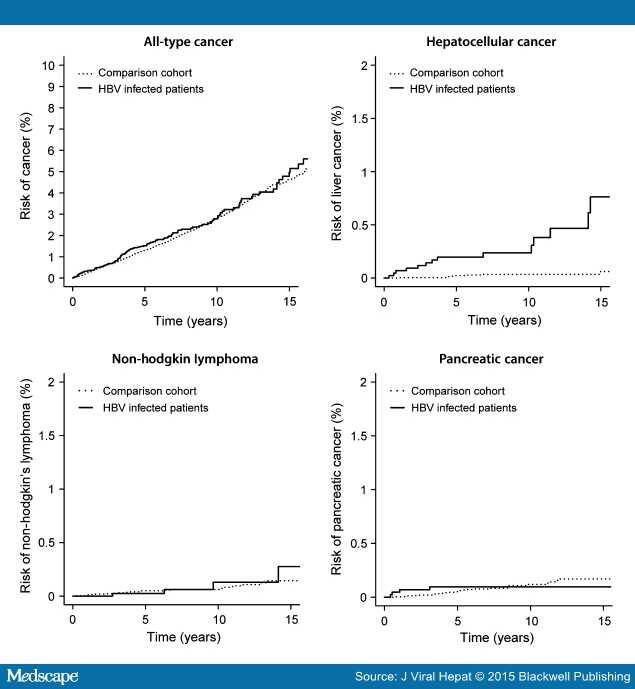
In this nationwide cohort study, an increased risk of HCC was observed in the HBV-infected cohort. However, patients infected with HBV did not have a higher risk of all-type cancer, NHL or PC compared to an age- and sex-matched population-based comparison cohort.
The strength of the present study is the identification and inclusion of almost all patients tested positive for HBsAg in Denmark who fulfilled inclusion criteria, as well as long-time and complete follow-up. Our initial analyses showed that the cancer incidence was much higher in the first 6 months after the first positive HBsAg test as compared to the rest of the follow-up period. This could indicate that patients more frequently were tested for hepatitis B during a cancer examination. Some cancer examination programmes in Denmark include hepatitis testing. To avoid this phenomenon of lead-in bias, date of inclusion was 6 months after testing positive for HBsAg. Another strength of our study is that our data allowed us to exclude HBV-infected patients, who had HIV or alcohol-related diagnoses, were tested positive for HCV antibodies and/or HCV-RNA, suffered from comorbidity or with non-Danish nationality. We therefore presume that our estimates are not confounded by these important factors.
A potential limitation of the study is the inclusion of patients with only one positive HBsAg test. Some patients may have had an acute HBV infection and cleared this during the observation period, leading to underestimation of the risk of cancer. However, as the results of the subanalysis of patients with two positive HBsAg tests at least 6 months apart were essentially the same as in the main analysis, the influence of this potential bias was negligible. Furthermore, we had no information on antiviral treatment, viral load, genotypes and route of transmission, all of which influence the risk of HCC and other cancer.[3,29] We excluded patients with non-Danish nationality to avoid confounding factors of different culture and ethnicity. Some patients may have had Danish nationality but still have non-Danish background resulting in a risk of confounding. We assume that patients with non-Danish background but Danish nationality may have partly adopted Danish culture thus limiting potential cultural confounding factors but not genetic confounding factors.
Recently, Sundquist et al.[10] have observed a 1.8-fold higher risk for all-type cancer among Swedish HBV-infected patients in a large cohort study (10 197 persons with chronic hepatitis B included). HBV-infected patients were identified in a nationwide Swedish hospital discharge register (from 1987) and outpatients register (from 2000). Therefore, Sundquist et al.[10] may have included patients with more morbidity and thus a higher cancer risk compared to the background population. Also, the HBV-infected patients in their study might have been followed more closely than the general population leading to surveillance bias. To address these issues, we performed subanalysis on HBsAg-positive patients, who were also diagnosed in the Danish National Patient Registry. We observed a 2.0-fold increased risk of all-type cancer among HBV-infected patients compared to the comparison cohort. The findings from this subanalysis suggest that the cohort of HBV-infected patients identified through discharge/outpatient register is a selected group of HBV-infected patients with more morbidity (selection bias), who are followed more regularly by physicians as compared to the background population (surveillance bias). Furthermore, Sundquist et al.[10] did not postpone the observation period from the date of hepatitis B diagnosis to avoid lead-in bias, which may result in a false increased risk of cancer among HBV-infected patients. Amin et al. found in a large Australian cohort study, no increased risk of all-type cancer among HBV-infected patients in agreement with our findings. Amin et al. included HBV-infected patients through a database including both hepatitis test results from laboratories and reports notification by medical practitioners, thus limiting the risk of selection bias and surveillance bias. Patients were included 1 year from the first HBV notification to avoid lead-in bias.[9] Thus, the inconsistency in the findings of risk of all-type cancer between Sundquist et al., Amin et al. and the present study may be explained by selection bias, surveillance bias as well as lead-in bias.
Studies have reported varying incidence of HCC among HBV-infected patients.[5–10] Most studies of risk of HCC are conducted in countries, where patients mainly acquire HBV perinatally with high viral load, little liver damage, and are considered to be in their immune-tolerant phase for a long time. Our data showed that the risk of HCC for HBV-infected patients was lower than reported in most other studies.[5–8,10] As we excluded patients with non-Danish nationality, many of our patients were infected with HBV during adulthood through sexual transmission. These patients are less likely to be in the immune-tolerant phase with high viral load. As the risk of HCC is found to depend on the level of HBV-DNA,[3] the assumed lower level of viremia in Danish patients may explain the lower risk of HCC in our study.
Within the last few years, several studies have suggested a higher risk of NHL for patients chronically infected with HBV.[10,13–15,30–32] A few of these comparative studies are limited on testing for HBV infection on or after NHL.[14,30–32] In high-endemic countries, two large Asian studies observed an increased risk of NHL of 1.58 and 2.63, respectively.[30,31] Both of these Asian studies lack exclusion of patients with HCV and HIV. A few studies regarding risk of NHL among HBV-infected patients have been performed in low-endemic countries. Yood et al.[13] have in an American study found a 2.8 higher risk of NHL. The study did not address potential lead-in bias. Sundquist et al.[10] have recently published results from a Swedish cohort of patients with chronic hepatitis B. They found a higher risk of 4.79 for NHL (patients born in Sweden). The study is limited by selection bias, surveillance bias and lead-in bias as described earlier. Amin et al.[9] have in an Australian study without these potential biases observed no higher risk of NHL among HBV-infected patients in agreement with our findings. In agreement with Amin et al., we did not find a significant association between HBV and NHL, but our 95% CI was relatively wide (0.42–3.55) and in our subanalyses with two positive HBsAg tests, there was a trend towards a higher risk (IRR 1.9, not significant). If there indeed was an association between HBV and NHL, not demonstrated in our data due to lack of power, the absolute risk of developing NHL is still low.
An increased risk of PC among HBV-infected patients has been suggested by Iloeje et al.[17] in a Taiwanese cohort study following 3930 HBsAg-positive patients in a prospective study (comparison cohort of 18 541 HBsAg-negative individuals). The association between HBV and PC was found only in patients with HBV-DNA >300 copies/mL..[17] We could not confirm an association of PC and hepatitis B in our Danish cohort of HBV-infected patients. This may be explained with the assumed lower level of HBV in the individuals in our HBV cohort as described earlier.
In conclusion, patients infected with HBV have substantially increased risk of HCC, but this patient population does not suffer from increased risk of all-type cancer, NHL or PC as recently suggested. We found a 17-fold higher risk of HCC for HBV-infected individuals, but a low absolute risk of only 0.24% in the decade following HBV diagnosis.
|
|



 发表于 2015-10-31 14:45
发表于 2015-10-31 14:45